
The Most Interesting Needle in the World?
Future treatments for hearing loss—including gene therapy—could come to rely on a tiny 3D-printed microneedle designed by a close-knit team of Columbia physicians and engineers.
What does it take to design a new needle for medical use?
When the needle needs to be much thinner and sharper than any commercially existing needle and designed to deliver treatments to a previously inaccessible tissue, the answer is years of collaboration between a close-knit team of physicians and engineers.
The needle’s Columbia creators—ENT surgeon Anil Lalwani and mechanical engineer Jeffrey Kysar—are convinced their ultrasharp and ultrathin device will soon become an essential tool in the way hearing loss and other conditions of the inner ear are treated. “It's not an exaggeration to say our microneedle could be key to precision medicine for the inner ear,” Lalwani says.
In an interview, the two discussed how they began their partnership a dozen years ago, what goes into designing a medical device, and why they think their microneedle will revolutionize treatments for hearing loss and other conditions of the inner ear.
Why does medicine need this needle?
AL: We’re now on the cusp of gene therapies that can restore hearing by regenerating cells in our ears that we lose after years of exposure to loud noises. But we really don’t have a way to deliver those therapies in a precise, predictable, and safe way.
That’s because these cells are inside an almost inaccessible container in the inner ear called the cochlea. The cochlea is a spiral-shaped, fluid-filled bone, the hardest bone in our bodies
There is a tiny membrane—about 2 mm wide—in the cochlea that could theoretically give us access. But the membrane invariably rips when you try to make an opening with standard surgical tools. When that happens, you could permanently lose your hearing and sense of balance.
So that’s one reason we’ve been working on this microneedle: to introduce therapies into the cochlea without ripping the membrane.

Cells in the cochlea after injection via the microneedle of a gene therapy vector (bottom row) and a control solution (top row). Image provided by Anil Lalwani and Jeffrey Kysar/Columbia University.
The other is to use the needle to remove liquid from the cochlea for the diagnosis of inner ear disorders, like Meniere’s disease, which causes dizzy spells, nausea, and hearing loss. By sampling the liquid in the inner ear, we may be able to understand Meniere’s better, which will also help us find better treatments in the future.
How did the two of you start collaborating?
AL: We actually had our meet-cute or cute-meet, whatever that's called, through two of our postdocs, who were friends. They realized we could form a really good partnership.
JK: I had imagined that doctors could access any place in the human body. But when I first met Anil, he told me that, no, the inner ear was pretty much an unknown entity: nothing could be injected or removed from it. That’s what captured my attention.
That Saturday, I think, I went to the bookstore and picked up a book on human anatomy. I then started looking in the biomedical engineering literature to see what was known about the membrane. And I found very little. How many unexplored tissues are left in the human body to study? This one had some very fascinating properties, both geometric and mechanical, so it seemed like a fantastic opportunity for me.
What were some of the challenges in creating the needle?
JK: So let me talk a little bit about the theory of why things break. That's the general theme of my research.
From an engineering perspective, you can think of the membrane as a tarp that’s been pulled tightly. If you put a really small hole in the tarp, that hole will not grow spontaneously. But if the hole is bigger than a critical size, it will grow spontaneously and rip the tarp. Engineering theory tells us that if we can introduce a hole in the membrane that’s smaller than this critical size, the membrane won’t rip.
We just had to make a microneedle smaller than that critical size, about the width of a human hair in the case of the membrane. It is also necessary for the needle to be ultrasharp in order to minimize damage to the tissue during the perforation process, which promotes healing of the membrane after the procedure.
We tried a lot of different ways to manufacture the needle. Not long after we started our collaboration, a 3D printing method became available and that was the enabling technology. Two photon photolithography allows a so-called voxel resolution of around 200 nanometers, about a 10th of a percent of the diameter of a hair, very, very small. With that we can print needles that are extremely sharp and are made from polymers, like the epoxy you can buy in a hardware store. Our needles are many times sharper than any commercially available needle.
We put a lot of time and effort into making sure that the needles are sufficiently strong. We had examples that broke, or the channels inside didn’t form properly, or the tip blunted. That’s part and parcel of what we do as engineers, figure out how we can improve the design.
How do you know these needles will do what you want them to do?
AL: We’ve done dozens and dozens of animal surgeries, and we've never seen any negative effects or hearing loss. The microneedle doesn't make a hole bigger than the size of the needle, and the hole heals within 48 hours or so.
We’ve also shown the potential value of the microneedle, since this field didn’t exist until we created the device.
In one of our most recent papers, we used the microneedle to inject a contrast agent into the inner year of guinea pigs so we could use MRI to look at the sizes of different chambers in the cochlea. That may assist us with diagnosing Meniere’s disease, in which the middle chamber becomes much bigger. Right now, imaging the human cochlea is difficult. If we can diagnose Meniere’s more accurately, that should lead to better clinical trials and ultimately better treatments.

With the microneedle, a contrast agent can be injected into the inner ear and can help physicians see changes in the cochlea that could help them diagnose conditions like Meniere's disease. Here, MRI images of a guinea pig cochlea reveal the cochlea's different compartments. Images provided by Anil Lalwani/Columbia University Vagelos College of Physicians and Surgeons.
In a second recent study, we show that we can deliver siRNA—a type of gene therapy—in a reliable, safe fashion, without causing hearing loss. We wanted to make sure that there's no toxicity of the vehicle [liposomes] itself, but also that the treatment is distributed throughout the cochlea.
What’s next?
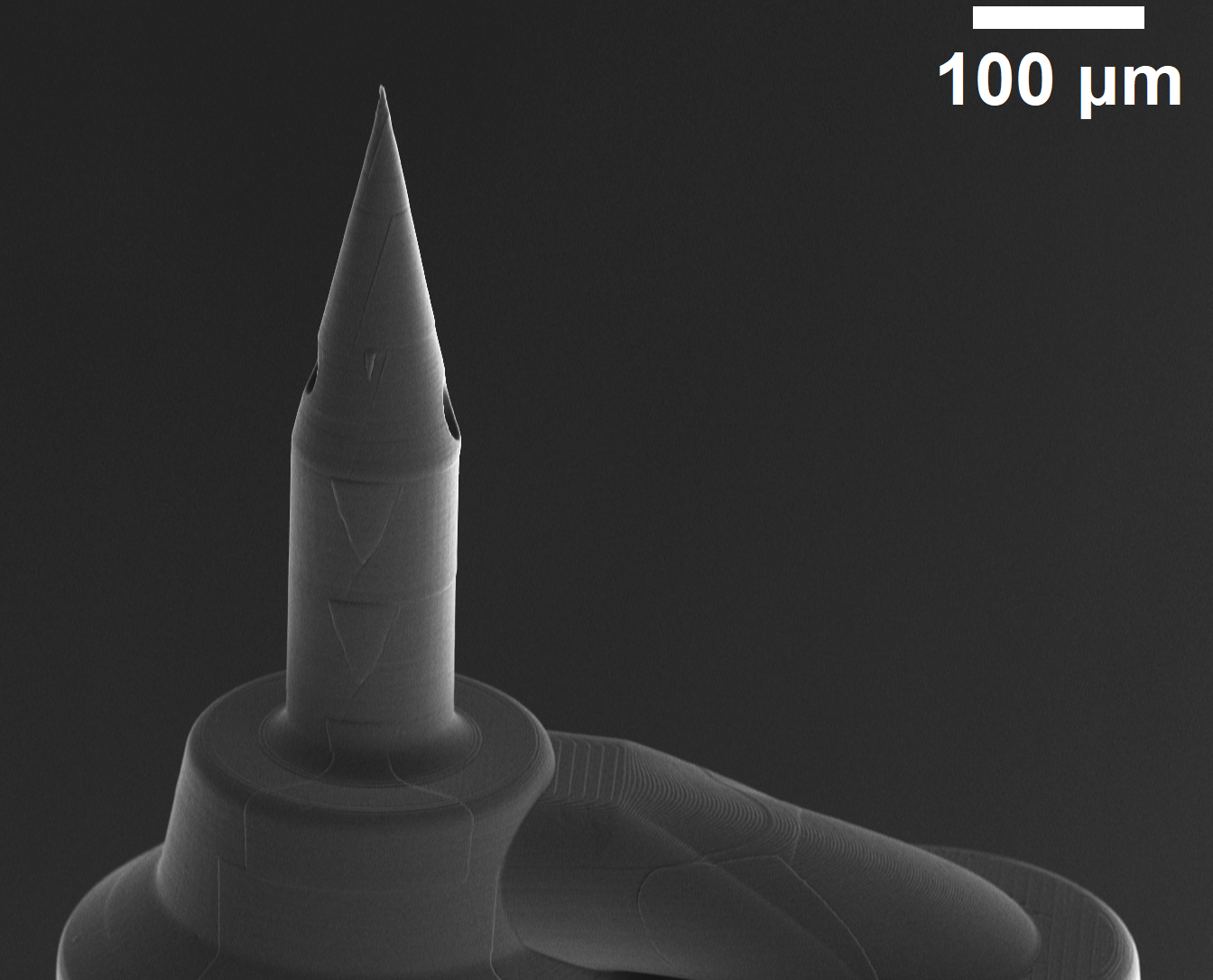
JK: With gene therapy, we're expecting that relatively large volumes of the therapeutic will need to be injected into the cochlea, and because the cochlea is a closed space, we’ll need to remove liquid as we inject. Otherwise, the pressure in the inner ear will increase and potentially damage the sense of hearing and balance. That’s why we designed the dual lumen microneedle, which will allow us to inject the therapeutic through one lumen and aspirate fluid through the other lumen simultaneously without changing the inner ear pressure.
AL: We formed a company about a year and a half ago now, called Haystack Medical, with the goal of commercializing microneedles. We're really excited about the next steps in translating this technology to use in people. Right now, we're talking to other companies creating gene therapies about using our technology. With the microneedle, you could potentially inject the therapy over and over again in the same person without causing hearing loss. You could see if the gene therapy is active, or if you need to readminister the material. That’s possible with the microneedle because it doesn’t scar or terminally damage the portal to the inner ear.
Overall, we think the microneedle is going to open the door—for the first time—to safe and reliable diagnosis and therapies for conditions that affect the inner ear.
JK: We are both very grateful to our outstanding team of students, postdocs, medical students, and our engineering colleague Elizabeth Olson, professor of biomedical engineering, as well as medical clinicians and surgeons who have been and are a part of our team.