
He Was Healthy. Then Excruciating Pain Took Over His Life.
Imagine the worst pain you’ve ever experienced. Your 10 on a 1-to-10 scale.
Now try to imagine it at 15.
That's how Dennis Pearsall explained his pain—which spanned five years before a recent surgery—to his family and friends. The first attack came out of the blue: “All of a sudden I had a jolt in my throat that went straight up into my eardrum and just exploded,” he said. “It was like someone had taken an electric prod and hit me. I didn't know what to do.”
He was standing in his office in Traverse City, Michigan, conversing with colleagues at the time. He had no previous ear, nose, throat, or head injury that might explain the attack. He was healthy and happy. Life was good. That was early spring 2017.
Over the next few months the attacks recurred, each marginally more painful and longer than the previous, five seconds to six, to 10, to 30. They were not regular or predictable but always connected to something going through Pearsall’s throat: cold drinks, food, air when talking. It felt like swallowing shards of glass. He saw an ENT. A comprehensive exam showed everything visible was normal.
For a few months Pearsall had a reprieve. Then came an attack so frightening he returned to the ENT. Again, a comprehensive exam could not find an issue. But the ENT had a probable diagnosis: glossopharyngeal neuralgia.
Glossopharyngeal neuralgia
The doctor explained the condition: When the glossopharyngeal nerve, which runs from the brain through the neck and throat to the jaw, is wedged against an adjacent blood vessel, excruciating pain can develop. Little else is known about it, but two treatment options were known to help—a drug and vascular decompression, a surgical option that separates the blood vessel from the nerve.
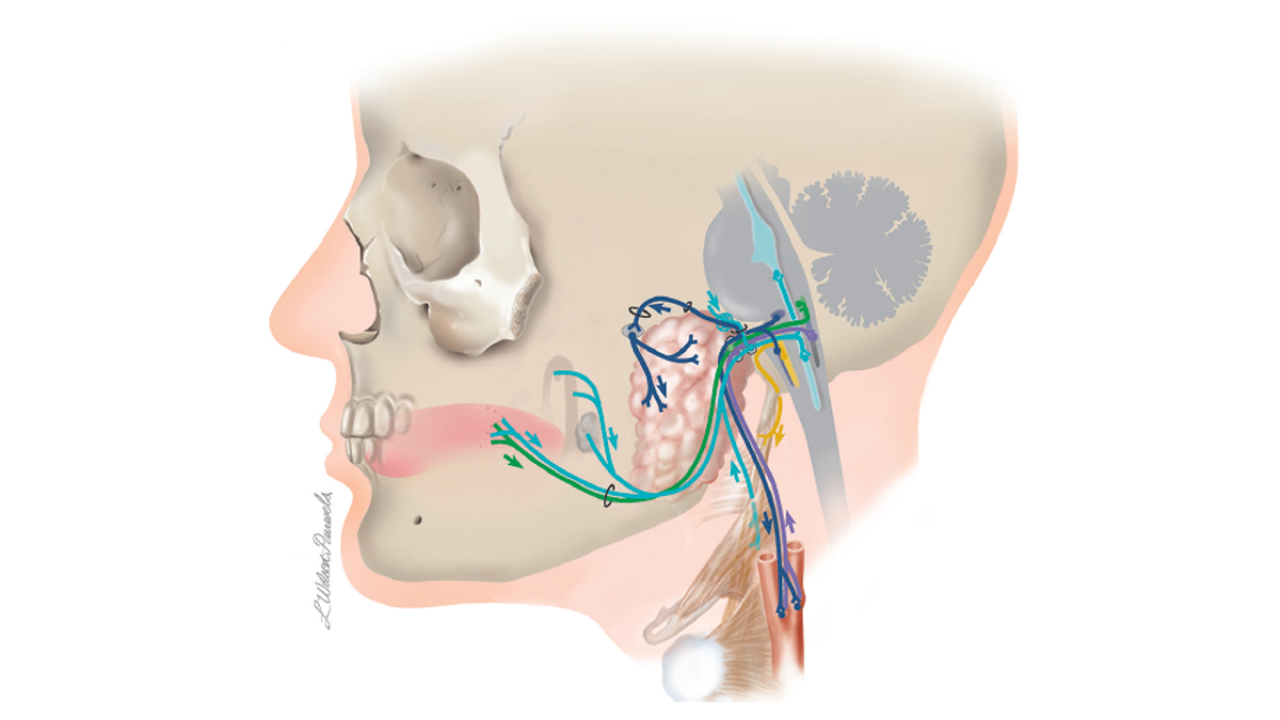
Glossopharyngeal neuralgia. People with glossopharyngeal neuralgia have attacks of severe pain in the throat, ear, tongue, and tonsils. Many describe the pain as a deep shock that extends from the back of the throat to the ear and feels like being electrocuted. The cause of glossopharyngeal neuralgia is not fully understood but is thought to be an irritation of the glossopharyngeal nerve, shown above. Fewer than 5,000 people in the United States have glossopharyngeal neuralgia. Illustration from "Cranial Nerves: Function and Dysfunction," 3rd edition.
Although the attacks continued to increase in duration and severity, brain surgery was something Pearsall was not ready to do. He took the drug and it appeared to work. He did not have another extreme attack for months. He paid attention to possible triggers, like ice, and avoided them when possible. But nothing could stop the progression.
Daily pain attacks

At the end of 2019, Pearsall and his family began researching options, attempting to find someone—anyone—in the surrounding states who could effectively treat the increasingly awful attacks, each lasting for at least one minute and happening daily for weeks at a time.
“I don’t like to exaggerate but this pain brought me to my knees,” says Pearsall. “It just takes your breath away. I would grab whatever I was near. The strain on my body—throat, ear, neck, my heart—was excruciating. It's the most unbearable thing that I can think of. When you have this pain you're helpless because there is absolutely nothing that you can do that will help.”
On Sept. 15, 2022, Pearsall went to an emergency department following the onset of an attack that did not cease. He felt like he was continually being stabbed at the back of the throat. Before being admitted to the hospital, he was in a waiting room with other patients for more than eight hours. He involuntarily hollered in pain. The memory gives him pause. “I felt stupid. The pain, the emotion, in a room full of so many other people.”
Attending physicians did their best to ease the pain and suffering they did not understand. A complete brain MRI revealed no tumors and nothing else doctors could discern. After a few days, Pearsall went home.
“You do not think you can get through it”
Because it is so rare, most doctors do not recognize glossopharyngeal neuralgia or confuse it with other conditions. For years, Pearsall and his family referred to a research paper describing the condition; his symptoms matched those described in the paper so closely that he was confident his ENT’s diagnosis was correct. But he did not have confirmation. And no matter how kind or sympathetic the hospital staff were, Pearsall says they didn’t have enough information to get him the help he needed, even after he offered the uncommon name to his symptoms.
At about five years, the paper predicted, the condition gets to a crescendo. It was five years now.
Pearsall could not swallow. He was severely dehydrated. He had attacks about every half hour, lasting up to 30 minutes.

"It completely took over and incapacitated me virtually in every respect, like when you're shutting down when you're dying. It filled me with anxiety. You wonder if you're just going down a slippery slope. You get to the point where you dread the next attack because you do not think you can get through it,” says Pearsall. So you do not eat, drink, or talk.
Pearsall went to the emergency department two more times over the next two weeks. He tried two painkillers and, ultimately, was swallowing liquid lidocaine near hourly for less than 10 minutes of relief, then immediately taking more to minimally function. Every non-lidocaine swallow triggered an attack.
Then, what Pearsall calls miracle No. 1 happened. His son got a referral to Raymond Sekula Jr., MD, a brain surgeon at Columbia University Vagelos College of Physicians and Surgeons, who specializes in cranial nerve disorders. Sekula has performed more than 2,000 microvascular decompression surgeries and is responsible for the procedure’s refinement.
Same day surgery. And relief.
To Sekula, Pearsall’s son’s description of his father’s experience and despair was both disturbing and familiar from previous patients. Sekula told Pearsall he could almost certainly alleviate the pain and offered to do so immediately.
Insurance and travel arrangements created delays, but with the support of his primary care doctor, Pearsall was on a plane to New York City four days later. He was told Sekula was the best and had performed hundreds of related surgeries. But he never expected the degree of professionalism, skill, and compassion that happened next.
Reviewing the MRI sent from Michigan, Sekula confirmed Pearsall’s glossopharyngeal neuralgia diagnosis. It was Oct. 6, 2022, five and a half years after his first attack.
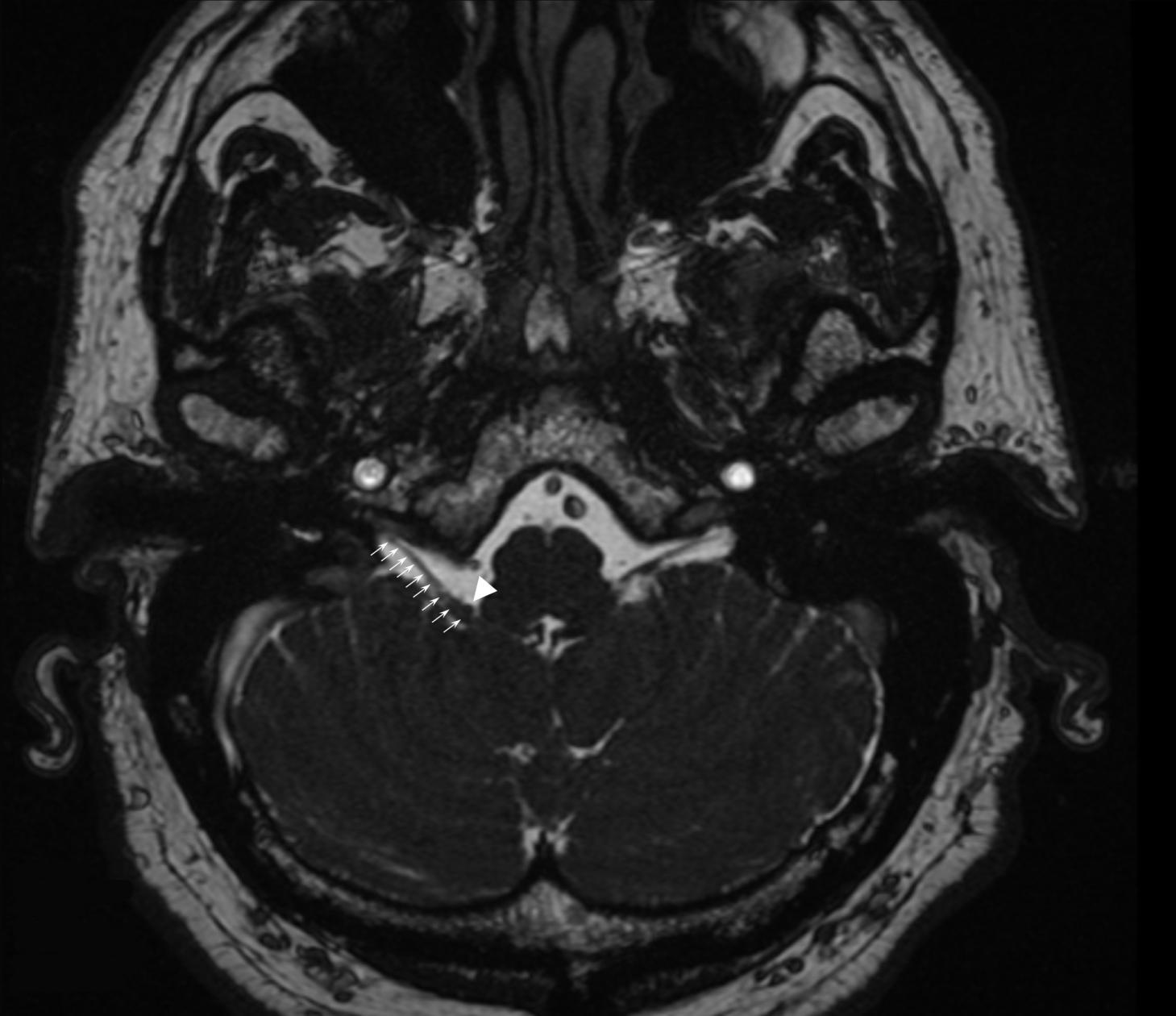
The patient's MRI showed an artery in the brain was compressing the glossopharyngeal nerve and pointed to a solution: microvascular decompression surgery. The arrowhead points to the artery. The line of arrows points to the nerve. Image courtesy of Dennis Pearsall.
“I was in such bad shape; my wife and son were doing the talking for me,” says Pearsall. “But we looked at the MRI and Dr. Sekula showed us the artery which was compressing my glossopharyngeal nerve on the right side. He could see what no one else could.”
Then Sekula explained the options: Have surgery as soon as possible, with a 90% chance of success, and a small risk of stroke, heart attack, loss of taste, or swallowing problems; wait to have surgery; or do not have surgery and likely be on a feeding tube for the rest of his life, which may not be very long.
For Pearsall, the decision was clear. He just needed to wait a week for time on Sekula’s surgical calendar.
Sekula, who was scheduled to be across the country the following day to teach a surgical course for fellow neurosurgeons, says Pearsall’s state—the end stage of glossopharyngeal neuralgia, when someone cannot mentally or physically take any more—was difficult to witness. “He was in agony. I didn’t feel right about having him wait with that much pain,” says Sekula.
After consulting with colleagues, Sekula offered to clear his schedule and operate that day.
Pearsall’s surgery was a success. He has been free of cranial nerve pain since. He lost his sense of taste, but it’s slowly returning. That’s a happy ending for most anyone but there’s more to this story, he says. “My experience at Columbia and with Dr. Sekula was lifesaving. I am so thankful. What I experienced with Dr. Sekula and his team just doesn’t happen, and yet it did. His unbelievable personal compassion and commitment to helping people with this type of condition is truly special.”
Pearsall says he is talking about his experience so he can reach as many people suffering as he can. “Glossopharyngeal neuralgia is a dead-end condition, but you can be helped, and you need to deal with it sooner rather than later. It doesn’t get better. If I had to have the surgery again tomorrow, I wouldn't even hesitate with Dr. Sekula in control. I’m forever grateful.”
References
Raymond Sekula, MD, is a neurosurgeon and professor of neurological surgery at Columbia University Vagelos College of Physicians and Surgeons. He is a world-renowned leader in minimally invasive brain surgery, devoted exclusively to cranial nerve disorders such as trigeminal neuralgia, hemifacial spasm, glossopharyngeal neuralgia, acoustic neuroma, and other skull base disorders. He also treats intraventricular tumors. He has performed more than 2,000 microvascular decompression surgeries.
Top image from Getty Images.