
The CRISPR Revolution: What You Need to Know
5 Questions About Gene Editing with Samuel Sternberg
Just a few years ago, CRISPR was known as a quirky way bacteria defended themselves against viruses, of interest to a few biologists and yogurt companies.
That’s when CRISPR expert Samuel Sternberg, PhD, now assistant professor at Columbia University Vagelos College of Physicians and Surgeons, started studying it as a graduate student in the laboratory of Jennifer Doudna. “CRISPR didn’t appear to have much relevance to human health, but it was a big, open playground with a lot of fascinating questions and no one working on it,” Sternberg says. “I remember presenting my work at conferences, dropping the word CRISPR and just getting blank stares.”
Now CRISPR seems to be everywhere in the scientific and popular press. The gene-editing technology promises to hasten the development of gene therapies: Europe’s first CRISPR trial got underway last year and U.S. trials for sickle cell and rare cancers received the go-ahead from the FDA. Popular culture also took notice last year, with CRISPR making its Hollywood debut in the thriller, "Rampage," and roasted by comedian John Oliver as the “Microsoft Word of gene editing.”
And then came the “CRISPR babies.” Scientists and the public alike were shocked when He Jiankui, a researcher in China, claimed he had edited the genome of two baby girls to prevent future HIV infection. That revelation led many CRISPR experts to propose a five-year global moratorium on heritable genome editing in humans.
“CRISPR is poised to impact our society in a number of ways over the coming years, whether in agriculture, human health, or infectious disease. Only by understanding the basics of CRISPR–how it works, and what it does and doesn’t make possible–can the general public make informed decisions about the responsible use of gene-editing technology,” Sternberg says.
We recently spoke to Sternberg about CRISPR controversies and where the technology is headed. Last year, Sternberg started his own lab at Columbia University Vagelos College of Physicians and Surgeons, where he is fine-tuning CRISPR’s components to make it more efficient and less prone to error.
Can you give us a brief description of how CRISPR works?
It’s not a perfect analogy, but CRISPR resembles the “find and replace” tool in Word. In Word, you type the word you want to find in the search box; in CRISPR, we create an RNA molecule that searches for a specific sequence in the genome. In Word, you type in the replacement word; with CRISPR we send an enzyme to cut the DNA and a molecule that serves as a template to edit the DNA.
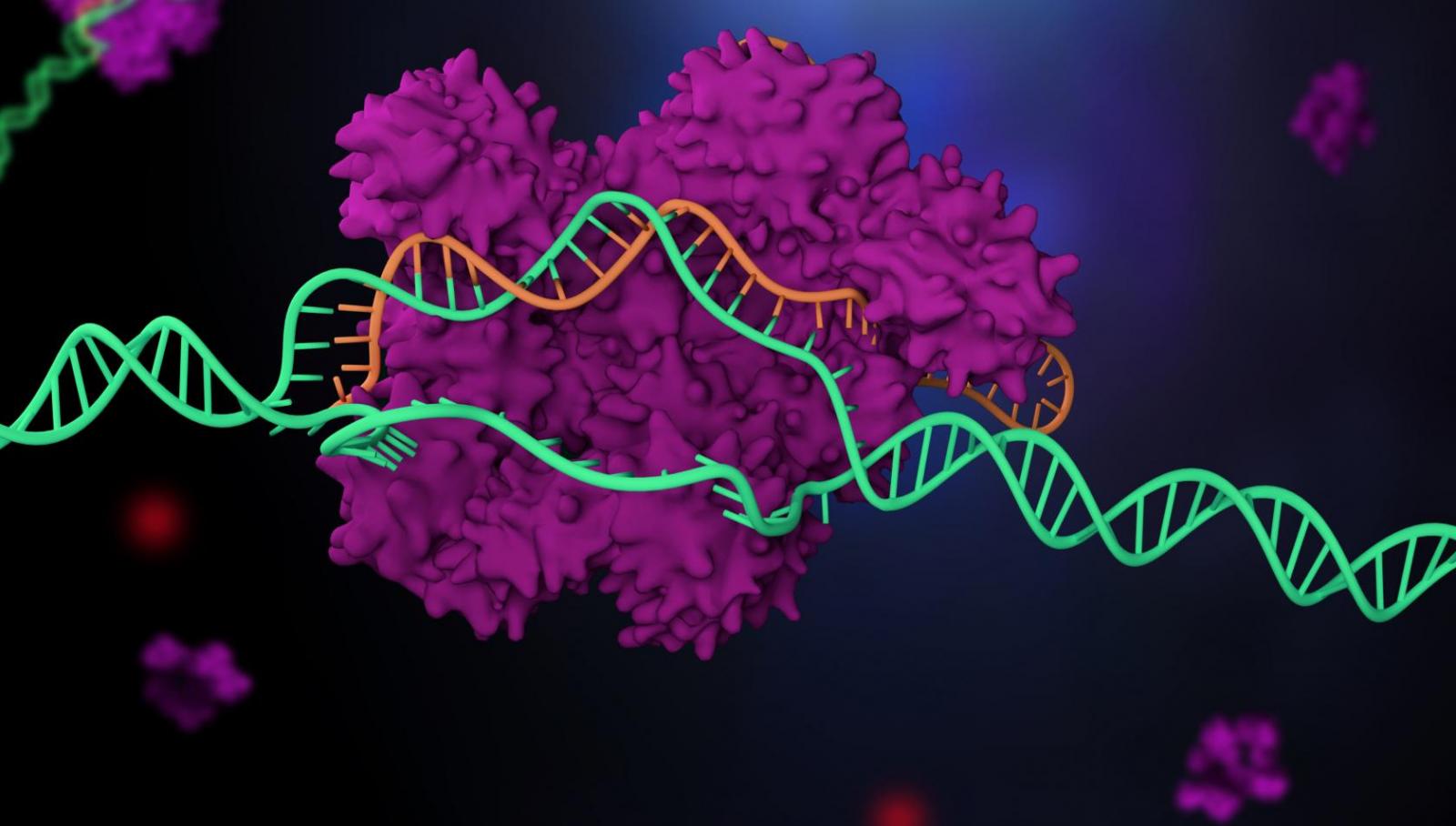
How CRISPR works. Typically in CRISPR, the Cas9 molecule (purple) uses a guide molecule (the orange RNA) to find a specific location in a cell's genome (green) to make a cut. Image: Getty Images.
Typically with CRISPR, the Cas9 enzyme is sent to the site to cut the DNA, but CRISPR can also drag along other enzymes. Some of the newer techniques use CRISPR not for gene editing, but to drag along enzymes that can turn genes on or off, or enzymes that can directly modify one letter of DNA to another letter without cutting the DNA strand, which can introduce errors. These techniques may be even more exciting than the original, simpler cutting version.
Why can’t we cure all genetic diseases with CRISPR right now? What are the difficulties in deploying CRISPR to fix an error in our DNA?
Controlling DNA repair is still a major bottleneck in developing gene editing for clinical applications. People say CRISPR is an editing tool, but CRISPR–Cas9 is really just the trigger for editing. It's the machinery that cuts DNA, but the way that the cut is repaired is still very hard to predict and control.
In other words, although it’s easy to make a random change in the gene, the hard part is controlling the exact change that's made. And so to treat a disease like sickle cell, converting the defective version of the gene back into the exact healthy copy, and doing so with an efficiency that is clinically useful, is still very difficult.
That's one reason why companies developing CRISPR therapies are targeting conditions where it’s not necessary to control the exact repair. So, in the case of sickle cell, instead of directly repairing the mutation in beta hemoglobin, one can instead introduce a mutation in a different part of the genome that is easier to execute and still has the desired therapeutic effect.
Delivery is another big challenge in living patients: How do you transmit these editing tools to complex organs and tissues? Treatments that remove cells from patients, modify them in the lab, and return them to the body–like blood cells for sickle cell treatment–circumvent major delivery barriers, so these treatments are getting the most attention.
Gene-editing tools have been around for decades. What’s special about CRISPR?
There just haven't been ways to manipulate genetic information precisely in higher organisms before. Genetic engineering in bacteria and yeast has worked amazingly well for decades. But in human cells, and in animal models like mice, we haven’t had the same kinds of tools.
The limiting factor was a way to target a specific part of the genome with precision, and that's really what CRISPR has made possible. CRISPR is a programmable machine: You essentially plug in the GPS coordinates of a precise location in the genome and then deliver gene-editing molecules to that site.
I think what is most powerful about CRISPR is this basic capability to send molecules to very precise locations in a staggeringly large genome. We have over 3 billion letters in our genome, dancing around inside the cell, but with CRISPR, we can now manipulate individuals letters with surgical accuracy.
With the so-called CRISPR babies, human embryos were edited so the change would be passed down to future generations. What was your immediate reaction to the news?
To be honest, I wasn't surprised. In our book ["A Crack in Creation: Gene Editing and the Unthinkable Power to Control Evolution"], Jennifer Doudna and I write about germline editing being an inevitable milestone that scientists are going to advance towards. There are reasonable arguments both for and against clinical use of germline editing. On the one hand, if CRISPR can help parents conceive a disease-free child where no other options exist, and it’s proven to do so safely, then one may ask why we shouldn’t pursue it. Yet the cases that fall into this category are quite rare, and one may argue that resources might be better spent on treating diseases in living patients.
In the case of Dr. He’s work, aside from the fact that there are already safer ways to prevent HIV transmission, which is what Dr. He was trying to accomplish, what's alarming is how cavalierly the work proceeded. His research team didn't even check to ensure that the genetic changes they made with CRISPR would have the intended outcome, before implanting the modified embryos.
One can attempt to reign in rogue actors, but the real challenge is whether some kind of international consensus about germline editing is even practical. The reality is that with a tool like CRISPR, any lab capable of doing in vitro fertilization can also edit an embryo’s genome. This technology has democratized genome editing so that it’s no longer something that only highly experienced individuals can implement.
The positive side of CRISPR is that for the first time ever, we can really think about tackling devastating human diseases in patients using highly precise "gene surgery," not to mention the researchers worldwide that can now use these tools in their experiments. CRISPR is driving research forward at a pace that would've been unprecedented just two years ago, and I think that's incredibly exciting.
With the CRISPR babies story, I'd say my biggest fear is not some doomsday scenario in terms of what terrible thing someone's going to do, but that unrestrained scientists, or even sci-fi movies like "Rampage," will sully the field and scare people. And then public opinion could turn against the technology.
What kind of CRISPR research are you doing now at Columbia?
What excites me on most days is the basic biology of CRISPR. CRISPR-Cas9 wasn’t invented in the lab, it was evolved over billions of years in the natural world. Newly discovered enzymes like Cas12 and Cas13 are gaining traction and those were revealed by going back to the basic biology of bacteria.
We want to mine the diversity of CRISPR-Cas systems in bacteria and see if there are more interesting tools that we can develop from these natural systems.
At the same time, one thing that attracted me to CUIMC was being in an environment where I’m much closer to physicians and clinical researchers. And so while we look to biology for inspiration, we can create and develop new tools that can be used to improve human health.
References
Samuel Sternberg is assistant professor in the Department of Biochemistry & Molecular Biophysics at Columbia University Vagelos College of Physicians and Surgeons.